
Mismatch Negativity (MMN) Case Study
Description
I've watched your MMN webinar. Thank you. Please can you help me evaluate the MMNs below, which are a 1 kHz frequent and 1.5 kHz rare stimulus.
Answer
Thank you very much for sharing your work.
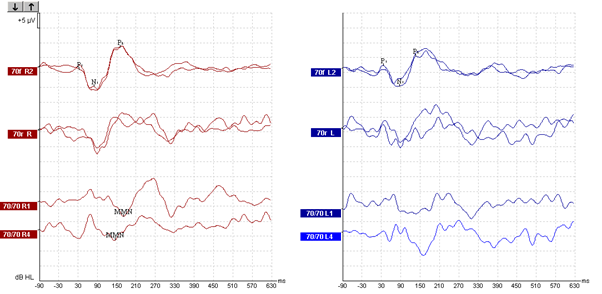
I believe I have some important feedback for you, which should help you achieve better results in future. I think the red traces in this example have some data that is clear enough to label as an MMN, but only just. I see the traces are organised according to my personal preference; I like to show the “frequent” traces at the top, the “rare” traces in the middle, and the difference traces together at the bottom.
If you refer to the red (right ear) traces then I would say that, on the face of it, the MMN labelled here is plausible for one of the two runs (70/70R1). If you see the vertical blue line that I have inserted then you can see that there is a downward deflection in the “rare” trace all lining up at 172ms latency, and there is also a normal N1-P2 complex in the “frequent” trace. The corresponding difference trace therefore also shows the downward deflection, and you have labelled this as the MMN. I would say this with reasonable certainty.
However, if we refer to 70/70R4 (the second of the two runs on the right) then we have MMN labelled at 146ms – but when you follow the black vertical line I have inserted then you can see there is no corresponding downwards deflection in the “rare” trace. Instead, there appears to be just a random coincidence of the way in which the frequent and rare traces had small kinks in them (mini peaks and troughs due to residual noise). I think what may have happened is the frequent trace has a mini peak and the rare trace has a mini trough at about the same latency, and together they have combined to produce a bigger deflection in the difference trace, and this has caused an apparent MMN in the difference trace. Another observation that supports this point is the difference in latency of the apparent MMNs between the two runs – one MMN is at 172ms and the other one (the false one, I think) is much earlier at 146ms even though this was two runs on the same listener, same test recording conditions and same stimuli. With all these factors the same I think you should expect a repeatable MMN at the same latency. I suggest the results on the left are inconclusive too, because of the apparently high residual noise.
My first key piece of advice would be to scrutinise your data in such a way that you don’t look exclusively at the difference trace. You must look at all three traces together to make sure that what you think is an MMN (viewed in the difference trace) does in fact correspond to the patterns of responses in the other two traces.
I suggest the major problem that you must overcome is signal-to-noise ratio in your rare traces. In order to do this then another key piece of advice is to record many more sweeps.
This is the major challenge of MMN. To interpret traces from an individual then what you need to do is present enough sweeps overall so that you get 150-200 sweeps in the rare trace. Then it should be about as clean (similar SNR) as you are currently getting in the frequent trace and should be a lot easier to interpret. Of course what this means is that you will end up with even cleaner data in the frequent traces. So, with a frequent-to-rare stimulus ratio of 85:15 (quite typical), with 150 sweeps in your rare trace you should end up with 850 sweeps in your frequent trace.
The challenge of course comes from the time needed to gather this many sweeps from one individual. You can work it out as follows; 850+150 = 1000 accepted sweeps at a rate of 0.6 sweeps/sec = approximately 28 minutes. But some sweeps will be rejected due to movement, eye blinks etc… so let us round it up to 30 minutes of recording, pragmatically. But if you want to do both left and right ears then this is 30mins x2 = 1 hour.
In your case you are already obtaining two traces per ear, per person. One alternative strategy would be to eliminate measuring in two separate runs. Instead do one long run in the same period of time. The usual purpose of doing two separate shorter runs in evoked potentials is to overlay the traces and show repeatability (i.e. residual noise, and SNR) by visually inspecting the correspondence between traces, but not only is this subjective but is obviously a hindrance here; the two runs are so short that there is little repeatability to show. Instead, do one long run. Now that you do not have two runs to visually estimate residual noise and SNR, an alternative is by referring to the pre-stimulus baseline (which should contain only residual noise, and when the noise is low the pre-stim baseline in the rare trace will be “flat” indicating residual noise is low). If using the research module then the Eclipse can log the individual sweep data and allow offline calculation of the variance within and between sweeps, to reveal the residual noise objectively.
Excellent general advice about using MMNs in clinical applications, including methods for optimizing recordings, is provided by Duncan et al., 2009.
References
Duncan. C.C. et al. (2009). Event-related potentials in clinical research: Guidelines for eliciting, recording, and quantifying mismatch negativity, P300, and N400. Clinical Neurophysiology 120, 1883-1908.
Presenter
