
Training in Anatomy / Physiology and Pathology
How to Diagnose SSCD with cVEMPs
Description
Are their rules for diagnosing superior semi-circular canal dehiscence (SSCD) using cVEMP?
Well there are certainly guidelines, as opposed to rules.
Perhaps it would help if we refer to the pathophysiology for interpreting such guidelines.
Patients with a dehiscent semi-circular canal (either the superior canal or another) exhibit a reduction in the impedance of the endolymphatic fluid to the flow of mechanical (sound) energy. In other words, sound energy moves more readily through the canal than normal – part of the so-called third window syndrome. (i.e. the dehiscence acts as a third “window” to the inner ear, the first and second being the oval and round windows which direct movement of mechanical energy through the inner ear fluid). A schematic of this effect is shown below.
Figure 1 shows a schematic of the normal configuration of the ear. Sound energy enters the inner ear via the stapes footplate inserting into the oval window. Inwards movements of the footplate result in a corresponding outwards movement of the round window to allow sound vibrations to propagate along the cochlear duct. Some amount of sound energy might propagate through the vestibular system (and can be used to elicit a VEMP), although normally the fluid impedance is high in this region so the sound intensity would have to be high in order to elicit a VEMP.

Figure 2 shows a dehiscent superior semi-circular canal. The effect of this third window is an increase in sound energy propagation and an increased cervical and ocular VEMP amplitude.
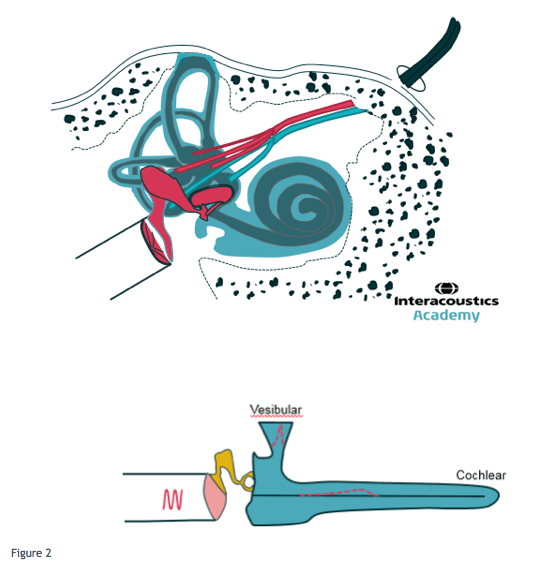
That is, although the VEMP itself is a test of otolith function, anatomically the sound energy introduced at the oval window during the VEMP procedure would propagate through the vestibule on route to the dehiscent canal. Simultaneously, less sound energy flows through the cochlear duct, which results in a related diagnostic phenomenon – pseudoconductive hearing loss.
Therefore, a larger than normal c/o VEMP amplitude may be expected at normal sound stimulation levels (e.g. 90-100 dB nHL). A related outcome to VEMP testing is that a response may still be present at lower sound levels than normal i.e. the VEMP threshold is reduced. A third possible outcome is that there will be an interaural asymmetry in VEMP amplitude (and threshold) – the affected ear should show an abnormally high amplitude and low threshold although this would only be the case if one ear was affected. If both ears were affected then the tester might see enlarged VEMP amplitudes and low thresholds but no significant interaural asymmetry.
For more information, including an overview of management of patients, please see Minor (2005)
References and caveats
Minor, L.B. (2005) Clinical manifestations of superior semicircular canal dehiscence. Laryngoscope 115, pages 1717 – 1727.
Presenter
